
The dangers of not knowing enough about COVID-19’s impact on women in Pakistan
The Government of Pakistan has begun publishing gender-disaggregated data on COVID-19 at a national level. One graph on the government’s Covid-19 website illustrates that men constitute 74% of observed cases so far (as of June 29th 2020). This is a significant aberration compared to worldwide trends and is one of the highest proportions globally. A WHO report on Gender and COVID-19 published in May 2020 explained: “A preliminary analysis of the data shows a relatively even distribution of infections between women and men, with some variations across age groups”. In effect, between a fourth and a fifth of possibly missing cases of testing among women needs to be explained.
Figure 1: Proportion of COVID-19 cases (male)
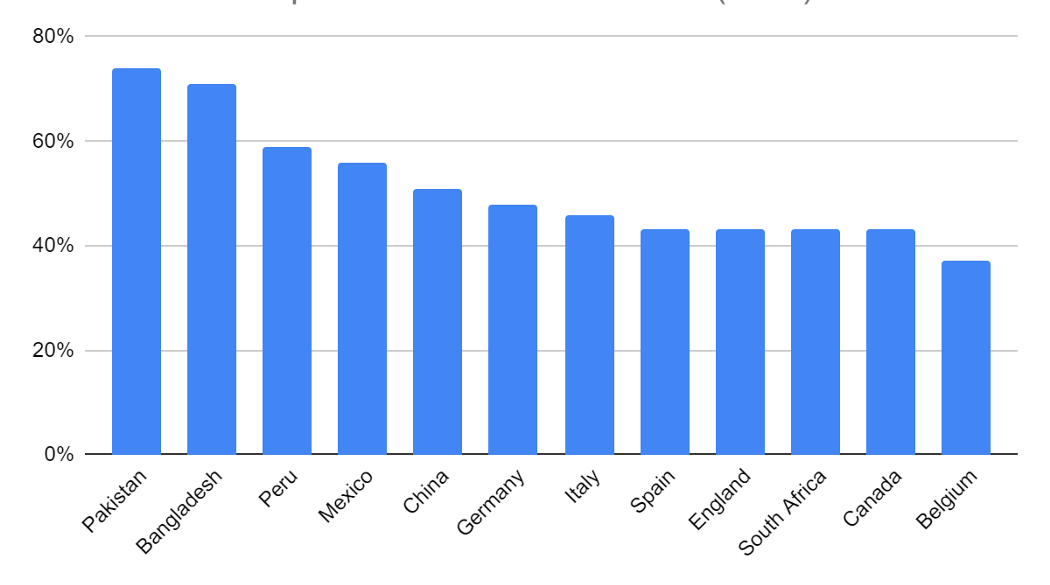
Data source: Global 5050
Data from a few cities in Punjab shows women make between one-fourth and one-third of all COVID-19 tests conducted in Pakistan. However, men and women test positive at roughly similar rates, with women testing positive a few percentage points more often than men.
We know how COVID-19 is transferred and why physical distancing is important. The more an individual is exposed to a wide group of people over time the more likely they are to contract it. In Pakistan, men have greater representation in the labour-force across sectors, greater participation in large congregations, particularly in mosques, and are simply more mobile than women. For example, men have a labour force participation rate of 77% compared to 21% for women in Pakistan. The 2012 JICA transportation study for Karachi found that the average number of trips per day for women is 0.71 compared to 1.92 for men. Similar numbers were found for Lahore in a 2010 transportation study and are expected to match other cities of Pakistan. The 2007 Time Use Survey in Pakistan echoes this reality within which 55% of women reported no trip in their day compared to just 4% of men.
An explanation for the high proportion of male cases of COVID-19 could then simply be the lower mobility of women in Pakistan because of which they are less exposed to the virus.
We would argue that it is not that women are getting infected less, but that they are simply being tested less for COVID-19 (Source: Punjab Health Department).
This makes logical sense. Even if women’s mobility may be constrained, men obviously live with women (barring perhaps migrant or seasonal workers). The average urban household in Pakistan has about seven individuals living and eating together in relatively small unventilated homes. Women are also often the primary caregivers in households making it harder for them to practice distancing from infected or potentially exposed household members. Spatial distribution of current observed cases also shows that infections are often reported within the same household. This effectively means that the risk of spreading indoors is significant. As such, if someone is infected and does not or cannot take sufficient precautionary measures they are likely to infect others they encounter or live with.
Compounding this further, according to data from the World Bank only about 50% of women report participating in decisions pertaining to their own healthcare and nearly a third stated that the decision to allow them to seek healthcare resides with their husband. Thus, even the decision to get tested or access healthcare does not always lie in the woman’s hands. The Pakistan Demographic and Health Survey further captured that roughly 28% of men (and 32% of women) agree that a husband is justified in beating his wife if she goes out without telling him.
Figure 2: Attitudes towards wife beating
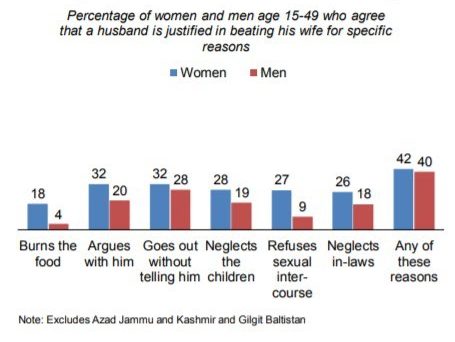
Source: Pakistan Demographic and Health Survey 2018
The implications should be clear. We know that the impact of COVID-19 will span a range of sectors from health, livelihoods, and mobility to household norms and roles and poverty level outcomes, but each of these components is expected to have significant gender-driven differences. One alarming outcome of cases not being sufficiently identified among women could be that the fatality rate will be much greater for women even though we may not attribute it to the disease. In addition, given that any targeted lockdown or isolation strategy depends on underlying observations of COVID-19 cases, missing observations on caseloads for women will result in a misallocation of resources, resulting in a significantly lower effectiveness of prevention measures. Lastly, a COVID-19 response strategy that fails to identify women as independent actors whose needs might differ from that of the household, will condemn women to be stuck within the constraints of the household. For example, one expected impact of COVID-19 on intra-household relationships are likely increases in domestic violence due to increased stresses. Without recognizing the unique risks women face in light of this pandemic, programming which needs development and deployment to mitigate these risks will be underfunded, or worse, never prioritized.
Some concrete efforts have been made by the Government of Pakistan. The publishing of gender-disaggregated data on COVID-19 cases is a laudable first step towards catering to men and women equally in the country’s COVID-19 response. The Government of Pakistan, provincial Departments of Health and Provincial Disaster Management Authorities are developing resources to provide emergency services to women prone to gender-based violence in collaboration with UNFPA. The UNFPA support also includes a socio-economic impact assessment of COVID-19 on reproductive health and health systems strengthening components with a focus on family planning and reproductive health services.
A complete COVID-19 response strategy has to centre women in managing this crisis in all dimensions. To understand the prevalence, pursuing affirmative random testing of women where there are high proportions of cases of males over females should become part and parcel of the COVID-19 testing strategy. This is supported by emerging evidence on the cost-effectiveness and viability of random testing, independent of gender, where observed incidence rates are low. To prevent disproportionately high infections among women, it will be crucial to identify community-based and household level solutions to maintain distance within households which includes men as part of the process of motivating additional testing. Data disaggregated by gender needs to be publicly available as currently planned to show variations by districts and allow for responses from the public and private sector to approach solutions with that information.
Moreover, published statistics without context will not elucidate the problem unless norms and behaviours around them are well understood. This article should make that clear. As such, ongoing research and COVID-19 response frameworks need to be designed to capture gender-disaggregated data, particularly attempting to understand and explain differences in knowledge, behaviour, perceptions, and barriers faced by women. In studying COVID-19 impacts in the immediate and long-term on key dimensions like health, food security, income loss, economic empowerment, and poverty, child health, domestic violence, remittances (domestic and international), or displacement, in the immediate or long-term, it is essential that women (and any relatively disadvantaged segment of society) are explicitly well understood and not subsumed within the unit of the household.
Supporting and developing homegrown innovations adapted for COVID-19 that specifically work on these challenges may be one additional approach to take. Lessons from longstanding efforts to identify cases of and combatting Tuberculosis could be useful. To complement this, the set of challenges may well exist in similar forms in countries like Bangladesh or Iran where the share of COVID-19 cases for men is 71% and 57%. Exchanging ideas and innovations across similar contexts, within or outside the immediate region, can be highly effective to fast track lessons and integrate applicable ideas into operations.
We echo ongoing calls for testing increases in Pakistan as COVID-19 cases continue to escalate. We would argue that this must be necessarily done through the lens of how different programs and policies will necessarily affect men and women differently across health, safety, and livelihood dimensions. An approach with this principle at the centre would ensure that women are not systematically neglected for testing, treatment, and support during this crisis. The consequences of not doing so will be dire for all Pakistanis.
Editor’s note: This article was first published in Medium.
Disclaimer: The views expressed in this post are those of the authors based on their experience and on prior research and do not necessarily reflect the views of the IGC.