
Overcrowding and pandemic risk hotspots in Rwanda
Proximity between people, otherwise known as population density, is the foundation of prosperity and productivity in cities. There is no empirical link between the spread of COVID-19 risk and city population density. However, when population density is not well managed and becomes overcrowding, the risk of COVID-19 and other contagious diseases, rises.
The COVID-19 pandemic has placed a spotlight on urban density, particularly in developing cities, where overcrowding in unplanned settlements makes it near impossible to practice adequate social distancing. Evidence has shown that overcrowding (Aligne, 2016) – and not density (Fang & Wahba, 2020) – is a risk factor for respiratory diseases such as COVID-19.
Urban density versus overcrowding
Even though many African countries have remarkably low pandemic numbers, overcrowding could be exacerbating the spread of the disease where it does exist. Moreover, overcrowding goes beyond COVID-19: Inadequate housing has other negative effects on public health, welfare, and the economy and is associated with a range of negative physical health impacts including increased instance of colds, asthma, influenza and diarrhoea, acute respiratory and gastrointestinal symptoms, cholera and tuberculosis (Neiderud, 2015). It has also been linked to depression in women, behavioural problems in children, lack of privacy, aggressive behaviour, psychological withdrawal and aggression in men, and other problems (Gray, 2001).
The pandemic risk posed by overcrowding also forces clarification around the implementation of the vital ‘densification’ pillar of Rwanda’s National Urbanisation Policy (See page 27, Rwanda Ministry of Infrastructure, 2015). Whilst the policy mentions the importance of public health, it does not mention overcrowding, so one important question is: how can Rwanda’s cities take advantage of agglomeration economies generated by densification – whilst avoiding overcrowding and its associated public health issues?
The study: Estimating the location of overcrowding hotspots in Rwanda
Rajashekar & Bower (2020) begin at the starting point that evidence shows that overcrowding, not population density alone, presents a risk for COVID-19 transmission. They then estimate the locations of overcrowding hotspots in Kigali and in five of Rwanda’s secondary cities. They define indoor overcrowding as little indoor floor space per person in a 100 metre square area, outdoor overcrowding as little outdoor built-up area per person in a 500 metre square area. They then measure these forms of overcrowding using International Growth Centre (IGC) data on building footprint and height, as well as other remotely sensed data on ‘built up area’ (European Commission, 2014) and WorldPop spatially disaggregated population data (World Pop, 2020). They also define a composite measure of overcrowding that includes both indoor and outdoor space. They argue that whilst evidence is clearest on the link between COVID-19 and indoor overcrowding, outdoor overcrowding – where houses are packed extremely close together – is also important to disease risk because it leads to a much higher frequency of both voluntary and unavoidable close interpersonal contact within a neighbourhood in both indoor and outdoor spaces.
Maps and tables of indoor overcrowding, outdoor overcrowding, and the composite indoor and outdoor measure, for Kigali and the secondary cities were created to illustrate this data spatially.
The findings: Overcrowding in cities and villages
Figure 1 shows the most overcrowded areas in Kigali – and therefore the country – on a composite measure that includes both indoor and outdoor overcrowding.
Figure 1: Composite measure of overcrowding in Kigali
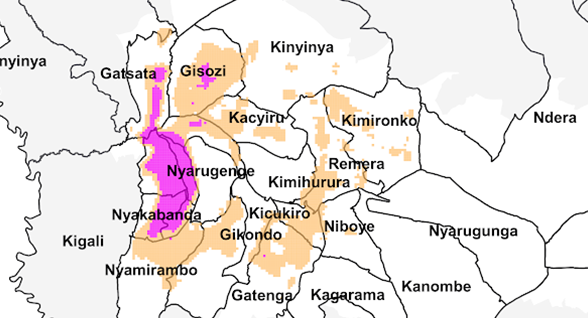
The authors find that the average level of indoor overcrowding (people per square metre of indoor floor area) is spread uniformly throughout Rwanda’s cities and throughout the country. On the other hand, as Figure 1 shows, outdoor overcrowding (population per square metre of outdoor built-up area) is concentrated in certain locations in Kigali city.
For example, one of Kigali’s 45 administrative “sectors” – Kimisagara – contains 42 of the villages (the smallest administrative unit in Rwanda) in the top 200 most densely populated villages in the city. Rubavu also contains significant overcrowding according to these measures, but in a very small area compared to Kigali.
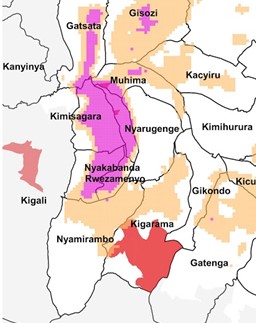
After the Government had instituted an initial period of national lockdown, then lifted it, they then implemented a policy of locking down a limited number of villages in central Kigali – six - that had exhibited COVID-19 cases, which lasted between June and August 2020. The authors overlaid the villages that had been locked down against the map of the most overcrowded locations, and found considerable overlap or proximity between the two as shown in Figure 2. This lends some degree of support to the hypothesis that COVID-19 poses the greatest threat in areas that are overcrowded in both an indoor and an outdoor context.
Figure 2: Villages locked down at some point between June and August 2020, mapped on to overcrowding
Policy implications
The Government could weight its package of COVID-19 testing and mitigation measures, and eventually vaccination, towards the most overcrowded areas.
The Government of Rwanda might consider higher levels of testing per capita for COVID-19 in the most overcrowded villages in the country - most of which are concentrated in a few sectors near the centre of Kigali, especially Kimisagara, Gitega, Muhima, Nyakabanda, Gatsata, and Rwezamenyo in this order. When a vaccine eventually becomes available, the Government might also consider higher levels of vaccination per capita in overcrowded areas, especially those that had to be locked down previously.
In the longer term, the densification pillar of Rwanda’s urbanisation policy should be pursued whilst avoiding overcrowding. This can be achieved by building above the first-storey, through funding, and building appropriate infrastructure.
The downsides of overcrowding do not nullify the densification pillar of Rwanda’s National Urbanisation Policy. Rather, international evidence emerging from the pandemic reinforces the conclusion that many cities that had very high population density also handled the pandemic extremely well: There is a crucial difference between density and overcrowding – the key is managing density well (Angel et al., 2020)
Well-functioning high density is usually not achieved through one-storey overcrowding, nor through high-rise blocks in contexts like Kigali. Simply building residential housing up to two, possibly three floors, is recommended, especially in areas closer to the centre. This increases indoor floor space – but can free up space for outdoor infrastructure too.
Connectivity is important too: Housing should be combined with roads that have adequate space for transit and well-designed public spaces. Evidence shows that effective grid structures and proactive planning for urban expansion can promote (without forcing) increased density over time, and protect public and private open spaces (Wainer et al., 2016).
In the longer term, access to water and sanitation is a fundamental investment to prevent the transmission of COVID-19 and other diseases, especially in the most overcrowded areas.
Water and sanitation, to enable frequent handwashing, is very important as a measure to prevent the spread of COVID-19 and other diseases as well as future pandemics (Kriticos & Mutizwa-Mangiza, 2020). It is estimated that ten percent of the global disease burden could be prevented through water and sanitation improvements, with large economic returns associated with increased health and productivity (Blake et al., 2020).